Monitoring and detecting safety signals at the regional level
The monitoring and detection system will be based on the work from the IPC Collaborating Centre, which will identify safety signals for priority products in VigiBase at the regional level:
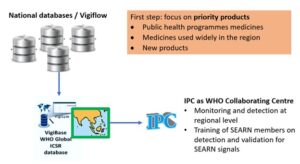
Priorities
As a first step, it was agreed to prioritize regional collaboration on medicines from the following category:
First step: Priority medicines:
- Public health programmes medicines
- Medicines used widely in the region
- New products
Among these categories, the main objectives of this surveillance programme would be to identify:
- Particularities due to populations/public health systems in the region, including for molecules which are already well known in other parts of the world
- New adverse drug events/new aspects in ADE for new medicines
- Substandard/falsified products with adverse consequences (e.g. due to microbiological or chemical contamination)
On this basis, a list of priority medicines was adopted. In addition, the Assembly recommended to include pregnancy adverse events in the priority list for monitoring /detection at the regional level.
List of priority medicines:
| Category | Active Substance(s) |
|---|---|
| Public health programmes medicines | Dapsone |
| Public health programmes medicines | Kanamycin |
| Public health programmes medicines | Isoniazid |
| Public health programmes medicines | Ethionamide |
| Public health programmes medicines | Ethambutol |
| Public health programmes medicines | Efavirenz |
| Public health programmes medicines | Doxycycline |
| Public health programmes medicines | Dolutegravir |
| Public health programmes medicines | Diethylcarbamazine |
| Public health programmes medicines | Darunavir |
| Public health programmes medicines | Lamivudine |
| Public health programmes medicines | Clofazimine |
| Public health programmes medicines | Clarithromycin |
| Public health programmes medicines | Chloroquine |
| Public health programmes medicines | Capreomycin |
| Public health programmes medicines | Bedaquiline |
| Public health programmes medicines | Atazanavir |
| Public health programmes medicines | Artesunate |
| Public health programmes medicines | Artemether |
| Public health programmes medicines | Nevirapine |
| Public health programmes medicines | Zidovudine |
| Public health programmes medicines | Rifampicin |
| Public health programmes medicines | Raltegravir |
| Public health programmes medicines | Quinine |
| Public health programmes medicines | Pyridoxine |
| Public health programmes medicines | Pyrazinamide |
| Public health programmes medicines | Primaquine |
| Public health programmes medicines | Paramomycin |
| Public health programmes medicines | Amphotericin B deoxycholate |
| Public health programmes medicines | Moxifloxacin |
| Public health programmes medicines | Miltefosine |
| Public health programmes medicines | Mefloquine |
| Public health programmes medicines | Lumefantrine |
| Public health programmes medicines | Lopinavir |
| Public health programmes medicines | Liposomal Amphotericin B |
| Public health programmes medicines | Linezolid |
| Public health programmes medicines | Levofloxacin |
| Medicines used widely in the region | Cefradine |
| New products | Fesoteroterodine |
| New products | Dalbavancin Hydrochloride |
| New products | Crisaborole |
| New products | Cannabidiol |
| New products | Asciminib |
| New products | Abrocitinib |
| Medicines used widely in the region | Mefenamic Acid |
| Medicines used widely in the region | Imatinib |
| New products | Imeglimin Hydrochloride |
| Medicines used widely in the region | Loperamide |
| Medicines used widely in the region | Dextromethorphan |
| Medicines used widely in the region | Ibuprofen + Paracetamol |
| Medicines used widely in the region | Olanzapine |
| Medicines used widely in the region | Phenylephrine |
| Medicines used widely in the region | Tetracycline |
| Medicines used widely in the region | Amoxicillin |
| Medicines used widely in the region | Paracetamol |
| New products | Prussian Blue Insoluble +/- Magnesium Hydroxide |
| Public health programmes medicines | Albendazole |
| Public health programmes medicines | Abacavir |
| New products | Trifarotene |
| New products | Treprostinil |
| New products | Tirzepatide |
| New products | Sovateltide |
| New products | Remifentanil Hydrochloride |
| New products | Relugolix |
| Medicines used widely in the region | NSAIDs |
| New products | Polmacoxib |
| New products | Plecanatide |
| New products | Plazomicin |
| New products | Niraparib |
| New products | Lobeglitazone Sulfate +Glimepiride |
| New products | Lifitegrast |
| New products | Lasmiditan |
| New products | Inclisiran |
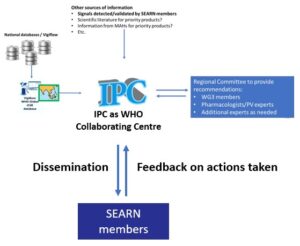
The assessment system will be based on recommendations provided by a regional committee composed of additional experts, based on safety signals detected either by the regional monitoring system or through other sources (such as signals detected/validated by SEARN members or the secretariat):
Objectives
To detect and assess safety signals at the regional level for priority products and on the request of one SEARN member or the SEARN secretariat, and advise SEARN Members on:
- The possibility of a causal relationship based on all available evidence,
- the need for risk minimization measures including regulatory actions (e.g. package insert and label etc.),
- the need for further studies to address remaining uncertainties.
Detection and validation at the national level
NRAs and national pharmacovigilance centres are responsible for detecting and validating safety signals at the national level. SEARN will support this work through the identification or development of training, guidelines and templates.
Prioritization
The IPC will review the preliminary assessment report from the SEARN member or secretariat to determine whether the signal requires further assessment, considering the potential impact of the on patients’ or public health and the risk-benefit balance of the concerned medicinal product(s).
If a signal was not prioritised, the IPC will initiate a discussion with the SEARN member or secretariat. If a divergence persisted, the issue will be brought to WG3 to decide the next steps.
Assessment
The organization which raises a signal is responsible for its assessment prior the regional discussions. Support may be arranged from Secretariat or another SEARN Member when the need arises. SEARN will support this work through the identification and development of training, guidelines and templates.
Recommendations, dissemination and feedback
The recommendations will be published on the website of SEARN and shared with members of WG3 and focal points.
NRAs will also be requested to provide feedback on how these recommendations were considered through the Monitoring and Evaluation framework.
Building on the strategy adopted by SEARN in 2023 to stimulate reporting, a regional preparatory session on supporting Member States in increasing vigilance reporting for medicines and vaccines was conducted on 13 October 2024, New Delhi, India. This session provided an opportunity for in-depth discussions and built consensus on key aspects of the regional strategy:
- Reporting objectives were agreed:
- 150 individual adverse drug events (ADE) reporting rate in million total population per year in 2027, and 300 in 2030 for medicines,
- 3 individual serious adverse events following immunization (AEFI) reporting rate in million total population per year in 2027, and 1 in 2030 for vaccines (completed with additional AEFI indicators)
- Key barriers to reporting were identified, as well as the key tools to prioritize in order to address these, which require close cooperation with critical stakeholders.
In line with the SEARN work plan and these discussions, a series of workshop with key stakeholders was developed to discuss means to increase reporting in the region. Meetings were organised with:
- healthcare professional regulators and associations on 9 April 2025
- hospitals (private and public) on 6 May 2025
- the industry on 4 June 2025
There was consensus among participants on the importance of increasing pharmacovigilance reporting in South-East Asia to ensure the safety of patients.
Tools and methods for increasing vigilance reporting were identified from the discussions, and those for which policy-level decisions would be required were identified. The prioritised methods and tools will be presented to the relevant policy makers during the next workplan for discussion and agreement on the next steps.
During its meeting in July 2025, the Assembly recommended to prioritise for further discussion with policy makers:
- Models/design of pharmacovigilance systems (e.g. regional pharmacovigilance centers, clinical guidance reporting from patients)
- Communication/engagement on pharmacovigilance / Yearly event
- Integration of pharmacovigilance in IT environment
- Including pharmacovigilance in initial / continuous training of healthcare professionals
- Including pharmacovigilance in accreditation/licensing/ performances of health establishments.