Scope and definitions
In 2021, the WHO Expert Committee on Specifications for Pharmaceutical Preparations adopted as an annex to its 55th report the Good reliance practices in the regulation of medical products: high level principles and considerations.
This document defines reliance as ‘The act whereby the regulatory authority in one jurisdiction takes into account and gives significant weight to assessments performed by another regulatory authority or trusted institution, or to any other authoritative information, in reaching its own decision. The relying authority remains independent, responsible and accountable for the decisions taken, even when it relies on the decisions, assessments and information of others’.
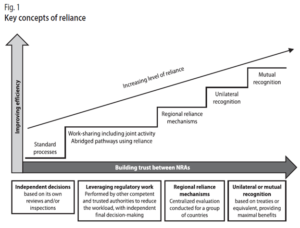
As Figure 1 describes, reliance may take many forms and be applied to varying degrees in recognizing or taking account of the assessments, decisions or other authoritative information of other authorities and institutions. While recognition may be seen as a special and more formalized approach to reliance, whereby one regulatory authority recognizes the decisions of another regulatory authority, system or institution, obviating additional regulatory assessment to reach its own decision. Recognition usually requires formal and binding legal provisions.
Reliance may be used in the regulation of any of the medical products in the scope of SEARN and for all regulatory functions, in the full life cycle of a medical product.
While the precise situations in which reliance may be used are to be defined at the national level, some conditions are required to enable reliance, including having access to sufficient information from the reference NRA such as full/public assessment reports in a common language documenting their regulatory decisions.
Converging on the definition of reference regulatory authorities in SEARN
The WHO Good reliance practices in the regulation of medical products: high level principles and considerations define a reference regulatory authority as a ‘national or regional authority or a trusted institution such as WHO prequalification (WHO PQ) whose regulatory decisions and/or regulatory work products are relied upon by another regulatory authority to inform its own regulatory decisions’.
The guidelines further highlight that ‘Each NRA should define its own strategy for an appropriate risk-based approach to reliance, which includes factors such as the type and source of products evaluated, the level of resources and expertise available in the NRA, the public health needs and priorities of the country and opportunities for reliance’.
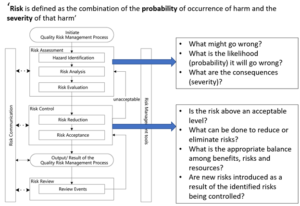
Further information on Quality Risk Management can be found in ICH Q9(R1) – 2021 and in the 2013 WHO guidelines on Quality Risk Management. The approach is summarized in the below diagram derived from ICH Q9(R1):
When identifying a reference regulatory authority, the below principles can be followed:
- It should be based on objective criteria, including evidence that the authority can be trusted (e.g. WLA, benchmarking, audit, accreditation, other information about the actions taken by an NRA), and the possibility to access the minimum required information in a language that is understood or can be easily translated.
- It should consider the capacity of the reference NRA to conduct the regulatory function independently (e.g. maturity level, or technical capacity to review further a dossier) and the capacity of the relying NRA compared to the reference regulatory authority to conduct the activities of a certain function (i.e. can the reference NRA do the assessment as well or better than the relying NRA? However, a minimum level of ML3/4 or WLA should be expected)
- It should be specific to one particular type of products and regulatory function (e.g. an authority may be ML3 for vaccines but not for medicines, or ML4 for vigilance but ML1 for marketing authorizations)
- It should be reconsidered regularly based on experience (e.g. for Marketing Authorizations, considering the frequency of substandard and falsified products).
- As a best practice, the relying NRA when applying reliance, should at least verify sameness. A checklist and guidance to conduct verification of product sameness for NRAs to use as reference can be found in the Appendix 2 of the 53rd report of the WHO Expert Committee on Specifications for Pharmaceutical Preparations (page 259) for Marketing Authorizations and Regulatory Inspections)
- It is recommended to publish on the NRA website a guideline on reliance, which defines the scope, criteria and principles followed to select reference authorities and how such assessment will be used, together with information which may be updated more regularly on which are the accepted reference regulatory authorities (for one particular type of product/function or type of decision). This will help stakeholders to comply with the NRA’s expectations.
Minimum information required for reliance
The below document was developed to support the implementation of this strategy. There would be 2 main usages of this information:
- Recommendations to guide relying countries on what is required as a minimum for them to be able to rely on other organizations.
- Recommendations to SEARN countries on what to publish/make available (in relation with AP3 information sharing and AP4 internal platform) in order to facilitate reliance from other countries on their own decisions.
Acknowledging that the implementation of these recommendations may require addressing practical and technical challenges, and in some cases further discussions and agreement of other authorities, the adoption by the Assembly of SEARN will be followed by an implementation period of two years.
The information identified in the below table intends to present the minimum information required for reliance. For reliance, the ultimate requirement is that the relying NRA should have sufficient trust in the reference authority to use the output of their work in their own regulatory decision-making system. Abridged assessment may require additional information.
The proposed SEARN convergence mechanism was developed following consultation in SEARN and studying experience from other regions (the EU, the ACCESS consortium), and a consultation of the industry.
Preliminary informal consultation with industry
A preliminary informal consultation in WG2 was organized on 21 April 2025 with industry to hear about industry’s perspectives on the proposed SEARN convergence mechanism, especially in terms of feasibility, expectations, and interest. Representatives included innovative manufacturers, generic manufacturers, as well as importers.
In general:
- The selected industry representatives were supportive of convergence initiatives and reliance, although on the longer terms they were calling for the development of regulatory recognition.
- These mechanisms are seen as having the potential of creating a significant impact for the industry through facilitating commercial flows of products between countries, while maintaining quality.
- In general, the industry called for waivers/simplifications/convergence of regulatory requirements between countries for marketing authorizations (including pharmacopeial requirements) and for regulatory inspections, as well as convergence of the accepted dossier formats.
- The industry also highlighted the importance of transparency, through clear procedures and requirements, from SEARN but also National regulatory authorities
- It was highlighted that to fully benefit the region’s industry, these mechanisms should consider generic products. The industry also invited to consider situation where such mechanisms could facilitate access to medical products facing shortages in one or several countries.
- Customs were identified as further important stakeholders important to facilitate export and import.
- To facilitate collaboration between manufacturers and importers, it was suggested to create a common platform e.g. through regular meetings, to discuss certain topics such as the issue of importers’ access to registration documents, especially in case of smaller quantities, or the need for quality agreement / technical agreement between manufacturers and importers
On the specific draft proposed SEARN convergence mechanism
- The selected industry representatives were generally supportive of the draft proposal.
- It was suggested that the Industry should also be able to suggest products to be considered as part of this mechanism, and to link it with the shortage policies
- Representatives highlighted the importance of providing very clear guidelines and procedures to industry and to link it with national guidelines on reliance
- The timelines for registrations were an important issue of concern and it was suggested to consider reasonable timelines for registration as part of this mechanism, e.g. 12-18 months, and to have clear guidelines about what happens if there is some delay at any stage of the process
- Clarity was also requested on whether health supplement and traditional medical products can be considered as part of this mechanism
- There was a request for participations of observers from pharmaceutical associations.
Further, NRA and partners representatives highlighted the importance of developing indicators for measuring the impact of this mechanism. Regarding vigilance, it was mentioned that there should be systematic access to RMP and that MAHs/applicants should consider regional component of RMPs also considering the diversity of healthcare systems in SEARN.
Revised proposed convergence mechanism on marketing authorizations
Please note that the below may still be subject to changes based on further consultations of SEARN members and stakeholders.
Context
SEARN is a volunteer association of the National Regulatory Authorities (NRA) of 11 countries in South-East Asia. While it was supported by Ministers of Health in the 2018 Delhi declaration on improving access to essential medical products in the South-East Asia Region and beyond, it is not supported by a common political / legal framework unlike other organizations (e.g. ASEAN).
At this stage, there is no consensus in SEARN on mutual recognition, and there are barriers to information sharing between countries. However, SEARN members expressed a desire to collaborate together on some marketing authorizations.
Key features of the proposed mechanism
The mechanism would take the form of virtual convergence workshops on priority products identified by SEARN Members, to facilitate reliance and access.
It would not be a mutual recognition mechanism, and no authorization would be automatically expected by the end of the process. However, it is expected that through common discussions, the positions from SEARN members on a particular product would be closer at this end of the process.
When feasible, it would build on other existing mechanisms, such as the WHO Collaborative registration.
The mechanism is intended to facilitate access to priority products in all SEARN Members.
Scope
Medicines and vaccines.
Virtual convergence workshop
For each product, 2 separate half day workshops would be organized for NRA assessors, experts committee members and SEARN members:
| Half -day 1 – Company workshop |
Half-day 2 - Authorities workshop (it may be organized a few days/weeks later) |
|
|
When a SEARN member already reviewed/approved the product of interest, the NRA is encouraged to present its assessment during the Authorities workshop.
In certain circumstances, grouped workshops may also be considered (e,g. for several similar products or for products covering the same need).
Proposed process and priority products

The relevant Working groups (WG2 for medicines and vaccines, and when applicable Ad hoc working groups), considering the definition of priority products, identify products of interest to SEARN to be proposed to the Assembly of the Members of SEARN or the Steering group. In addition, companies and industry associations may also propose some products to be considered under this mechanism.
The Assembly of the Members of SEARN or the Steering group, which may be consulted in writing, approves the products identified for the purpose of the convergence mechanism. When a product of interest to SEARN is identified, the secretariat would reach out to the company and a relevant reference organization to invite them to engage in the process.
Definition of a priority product
A priority product is defined as either:
1. a medical product intended to treat, prevent or diagnose
1.1. a serious life-threatening condition and which can address unmet medical needs such as:
- The absence or lack of a treatment option
- The provision of a significant improvement compared to available marketed products, such as evidence of increased effectiveness or elimination or a substantial reduction of a treatment-limiting adverse reaction
1.2. a disease or condition of public health concern for the region, such as certain cancers and infectious diseases.
2. Or, a medical product, the assessment of which requires rare expertise due to the complexity of the product and/or the disease addressed
3. Or, a medical product required to address a situation of shortage
4. Any other product as decided by the Steering group and/or the Assembly
Benefits and expectations for participating companies
The mechanism would provide an opportunity for companies to present their dossier and benefit from convergence between SEARN NRAs on the assessment of the dossier (E.g. position on granting MA, MA conditions and product information, questions to MAH). The company would benefit from improved knowledge about the NRAs expectations in the region and facilitated access to information on the submission requirements.
The mechanism is intended to facilitate access to priority products in all SEARN Members. Through participating in this mechanism, there would be a general expectation that access will be facilitated in all countries, either through application for marketing authorisation or facilitating access to access to full dossier and inspection / assessment / scientific advice report to SEARN NRAs (and if feasible local importers).
Benefits and expectations for SEARN Members
From the perspective of participating National Regulatory Authorities, these workshops should contribute to ensure quality decision making, facilitate the assessment process, build capacity through experience sharing, and eventually facilitate access to the products of interest.
In order to facilitate the implementation of the mechanism, SEARN Members are expected to reflect information about the SEARN convergence mechanism in their relevant national guidelines and/or public website. SEARN members should participate in the workshops and present their assessment when applicable, and provide the information required for the monitoring and evaluation framework. The NRAs should conclude their assessment within a defined time from receiving e.g. a valid marketing authorization application for a product of interest.
Review and engagement with stakeholders
To monitor the impact of the proposed mechanism and review it as required, SEARN will include dedicated indicators in its Monitoring and Evaluation Framework.
In addition, SEARN will regularly engage with representatives from manufacturers, generic manufacturers, as well as importers, and their associations to discuss the mechanism, its implementation, and address arising challenges.